Hormone Planning Period tasks
The following is a guide to the planning period for new (or newly transitioning) trans patients who have reached tanner stage V in pubertal development and are interested in hormone therapy (for options for pubertal youth, please refer to the updated Endocrine Society Guidelines1). It is more important that the tasks of the planning period are completed, rather than a certain number of visits logged or period of time elapsed.
Hormone Planning Period Checklist
Rationale for planning period
The planning period is important for:
- Establishing rapport with the patient
- Ensuring the patient has all the information they need to start hormone therapy
- Ensuring the patient feels prepared
- Offering additional supports to the patient as needed
Source
- 1. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline.[published correction appears in J Clin Endocrinol Metab. 2018 Feb 1;103(2):699] [published correction appears in J Clin Endocrinol Metab. 2018 Jul 1;103(7):2758-2759]. J Clin Endocrinol Metab. 2017;102(11):3869‐3903. doi:10.1210/jc.2017-01658
Patient history
Using respectful language
- Facilitate a trusting, open relationship by using respectful language
- Always refer to your patient by their chosen name and pronouns. If you are unsure, ask the patient how they would like to be called.
- It is also helpful to check in with a patient regularly about changes in their preferred name or pronouns and to encourage them to let you know if they change in the future.
- Use references that describe someone’s present identity (how they identify on that day), not their assigned identity.
Using a trauma-informed approach
Trans patients invariably experience some degree of minority stress, and many are exposed to gender-based interpersonal violence. Negative experiences in health care settings can further exacerbate the effects of this trauma. In addition to ensuring a gender-affirming approach to all trans and non-binary patients, it is encouraged that providers be familiar with and practice trauma-informed care. A 2018 review in
Source
- 1. Purkey E, Patel R, Phillips SP. Trauma-informed care Better care for everyone. Canadian Family Physician 2018;64(3):170-172
Questions to ask:
How would you like to be addressed? What name and pronoun would you like me to use?

General medical intake & medical history
This includes obtaining past records from previous provider(s), if this is a new patient.
Gender history
Speaking with clients about their history and experience with gender is not something that healthcare providers are typically taught during their training. It is, however, an important part of getting to know a trans patient and informs the discussion around the development of an individualized care plan. Reassure your patient that there are no ‘wrong answers’, nor any specific narrative that the provider is looking to hear. Not all trans people experience gender dysphoria/incongruence or display gender diversity in childhood; trans identities may emerge at any point in the life cycle.
Click to view possible questions to open a conversation about gender identity

Baseline data
Focused Physical Exam
A focused physical exam is generally recommended prior to the initiation of hormone therapy. The exam should include screening for problems such as hypertension, obesity, and active liver disease which may increase the risks of hormone therapy. A baseline breast exam and measurements (e.g. chest circumference at fullest part of the breast and areolar diameter) may be helpful for transfeminine patients, particularly those who may wish to pursue publicly-funded breast augmentation.
- For an overview of current MOHLTC-funded Transition-Related Surgeries visit the resources section on TRS processes
Keep in mind
Assess the level of comfort a patient has with a particular examMany trans patients have avoided medical practitioners because of fear of mistreatment or stigmatization, thus may not have had routine screening manoeuvres employed. A discussion about risks and benefits of a particular manoeuvre may be helpful. In some situations an exam can be deferred to another time and/or declined.
You can build rapport and increase a patient’s comfort by:
- Carefully explaining to the patient ahead of time why the exam is essential to the patient’s health
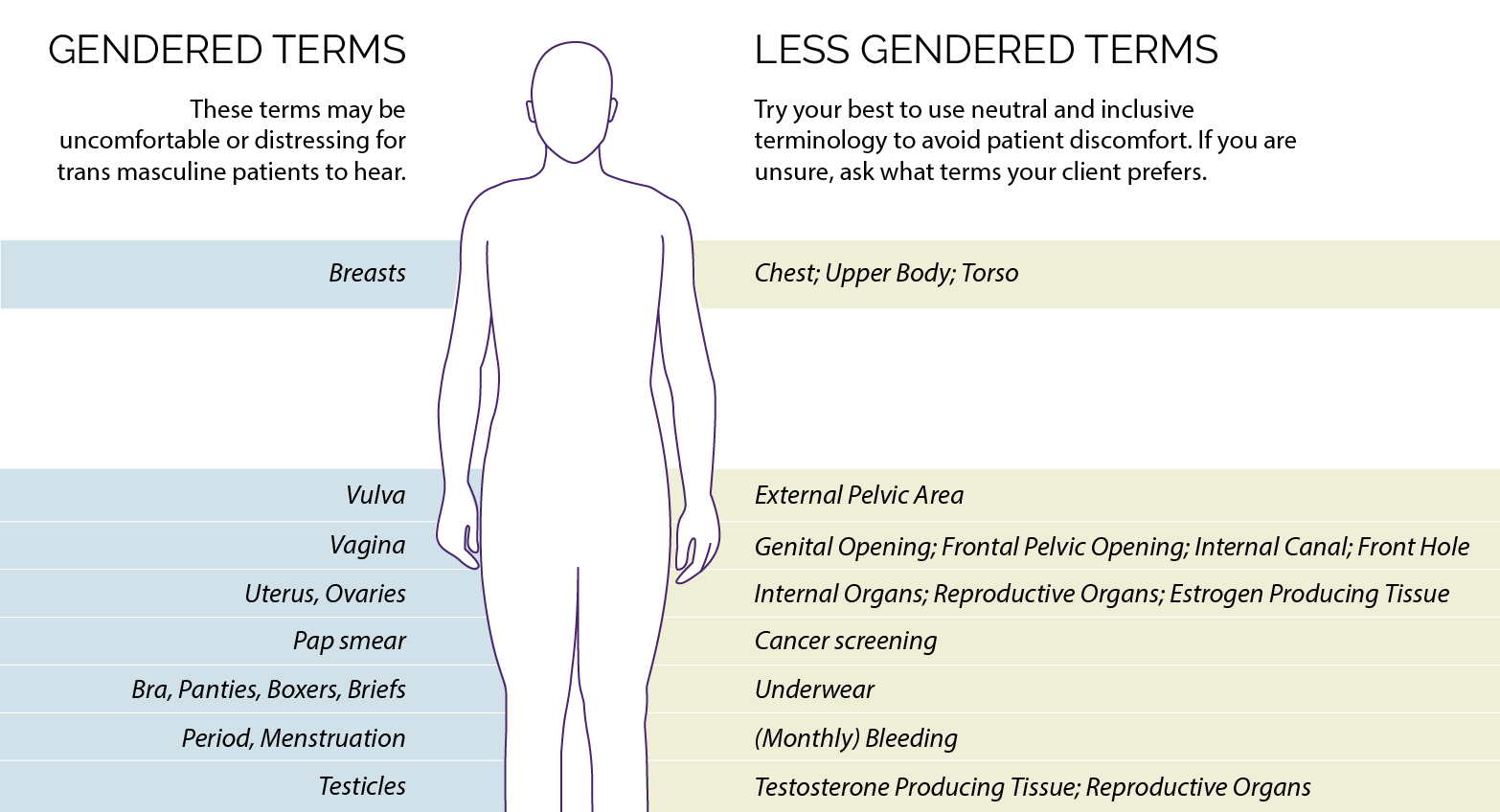
- Ask the patient if they have certain terms they would prefer you to use to refer to specific body parts.
Do you have any words to describe specific body parts that you would like me to use?
View suggested terminology that may be used with transmasculine patients
Vitals
Basline measures include blood pressure, height, and weight
Bloodwork
Laboratory tests are used to investigate for existing health problems such as liver dysfunction, high cholesterol, or diabetes. If present, these conditions should ideally be managed prior to or concurrently with starting hormone therapy. The values will also provide a useful baseline to help with the future monitoring for endocrine changes. The measurement of hormone levels may reveal whether any exogenous hormones are being taken; any major irregularities could also indicate an intersex condition.
View baseline bloodwork summary for transfeminine and transmasculine patients
Suggested terminology to use with transmasculine patients
Patient education and readiness
To learn more about each step, click on the items below:
What are the patient's physical transition goals?
Allow the patient to articulate their transition goals and expectations.
Does the patient have reasonable expectations?
Physical changes associated with hormones can be slow – it may take years to exhibit some secondary sex characteristics. Some features, such as underlying body structure, will not change with hormones.
It may be helpful to provide the patient with a copy of the estimated timelines for hormonal effects, while emphasizing that physiologic response to hormone therapy is highly individual. Please see the section on "Effects and Expected Time Course of Feminizing and Masculinizing Hormone Therapy" in the Quick Reference Guide below.
Quick reference guide for primary care providers (ENGLISH VERSION)
Aide-mémoire pour professionnels de la santé de première ligne (FRENCH VERSION)
View possible questions to open a conversation about realistic expectations
Does the patient hope to have a genetically-related child one day?
Discuss the effects of hormone therapy on fertility with the patient.
- Feminizing hormone therapy results in reduced testicular volume and affects sperm motility and density, which may be irreversible.
- Fertility may be permanently affected by testosterone hormone therapy.
Ask patients whether they hope to have a genetically-related child one day. If so, ask about their interest in banking their sperm or eggs.

Options for fertility preservation
If a patient suspects they may wish to have genetically-related children in the future they should be advised to bank sperm prior to starting hormones. Sperm cryopreservation following ejaculation is the simplest and most reliable form of preservation, but other procedures, such as testicular sperm extraction (TESE) can be considered when ejaculation is overly burdensome or difficult. Patients may also attempt conception or undergo fertility preservation following the suspension of hormone therapy for three to six months, as testicular function may recover to a variable degree.
While many transmasculine people have intentionally become pregnant after discontinuing testosterone to pursue pregnancy, patients may wish to consider postponing testosterone initiation if they would like to become pregnant in the near future. Counselling regarding fertility preservation should occur prior to starting hormones. While ideally completed prior to starting hormones, fertility preservation can also be performed following (temporary or permanent) discontinuation of testosterone. Fertility preservation involves cryopreservation of either ova or of embryos created via fertilization with sperm from a partner or donor. This involves harvesting of ova following ovarian stimulation through administration of female hormones, as well as multiple transvaginal ultrasounds and a transvaginal procedure to aspirate the ova. This often represents a substantial physical and psychological burden for transmasculine patients.
Discuss the risk of pregnancy and options for contraception
Discuss pregnancy risk and options for contraception with the patient. It’s important to have a discussion about sex and birth control.
View questions to open a conversation about sexual practices
Options for birth control
Transfeminine patients should be cautioned regarding the need for birth control if sexually active with partners who may become pregnant, since hormonal impact on fertility in transfeminine patients is variable.
Testosterone therapy does not prevent pregnancy even if amenorrhea is achieved. The patient must take precautions against becoming pregnant while taking it. Patients who are sexually active with people with sperm should be counselled on contraceptive options including progesterone-only contraception or an intrauterine system/device (IUS/IUD). Anecdotally, it may be easier to insert an IUS/IUD prior to initiating testosterone, due to the subsequent atrophic changes of the vaginal and cervical tissues1. If testosterone is initiated, the provider should check in with the patient periodically regarding their sexual behaviour and reiterate the necessary precautions should the patient become sexually active with people who produce sperm.
Source
- 1. Bachmann, G.A., & Nevadunsky, N.S., 2000
Gender transition can be a phase of significant adjustment in the life of the patient. Like any major life stressor, the aim is to ensure the patient has supports that facilitate healthy adjustment.
Individual support
The patient may benefit from individual therapy with a trans-positive therapist with whom to discuss concerns about the transition process and to receive psychological support. Though not a requirement for the initiation of gender-affirming hormone treatment, we encourage patients to discuss the transition with family members and friends as they too will have their own reactions and be affected by the patient’s transition.
A list of providers, including mental health professionals, with knowledge and experience working with LGBT2SQ individuals may be found through Rainbow Health Ontario’s online service directory.
Go to list of providers
View possible questions to open a conversation about psychosocial readiness
Peer group support
When available, we recommend the patient consider a peer support group setting (for example Sherbourne Health's Gender Journeys).
Gender Journeys is an 11-week program in which individuals can explore their gender identity, learn about different aspects of social and medical transitioning, and build communities. Gender Journeys was developed at Sherbourne Health and has been running since 2005. Gender Journeys groups are now offered in several cities throughout the province.
Common requests
Your patient may seek assistance from you in order to access services and supports they may need. Below are some common support letters that primary care providers are frequently asked about.
Note: while we recognize that indicators of gender, rather than sex are being discussed, Ontario’s documentation consistently uses the term ‘sex designation’; thus for simplicity we will use this term here.
Changes to gender markers on Ontario health cards
As of June 2016, sex designation is no longer displayed on Ontario health cards. Upon next renewal, cardholders will receive a card that does not indicate sex. If a patient wishes to get a health card without a sex indicator before their regular renewal date, they can get one by calling 1-866-532-3161 (TTY 1-800-387-5559) or by visiting any ServiceOntario centre. There is no fee to get a new health card.
It should be noted that sex designation remains part of the information associated with the card. If an individual has already changed the sex designation on their Canadian Citizenship document or other OHIP-eligible immigration status document, they can use that document to change their OHIP sex designation. Alternatively, the applicant can write a declaration along with the letter from their primary care provider to support the change of OHIP sex designation. Currently, there is no option for a non-binary sex designation (eg. 'X') to be associated with a person’s OHIP card.
Changes to gender markers on Ontario Driver's Licenses
In early 2017, driver's license holders will be given the option to display an 'X' on their card as their gender designation if they do not exclusively identify as a girl/woman or boy/man.
Additional information can be found at:
Discuss and ensure your patient demonstrates a good understanding of the potential benefits, precautions and side effects of hormone therapy. Beneficial effects, risks and precautions of the individual hormone treatments can be found in the feminizing and masculinizing hormone therapy sections of this guide.
-
Checklist for Patient Review – Initiation of Feminizing Hormone Therapy
-
Checklist for Patient Review – Initiation of Progestin Therapy
-
Checklist for Patient Review – Initiation of Masculinizing Hormone Therapy
Does the patient possess capacity to consent?
As with any other medical intervention, patients must demonstrate an understanding of the risks and benefits of hormone treatment. Obtaining informed consent is a process that primary care providers engage in daily, and when prescribing hormones to trans patients, the same basic principles apply. Questions may arise around capacity to consent in individuals with cognitive or developmental disabilities, significant mental health and substance use challenges, or younger patients. Since there is no specific age determining when an individual is eligible to provide consent for medical interventions in Canada, it is determined on a case-by-case basis and at the discretion of the provider.
Review medication options with patient
Discuss the different treatment options with the patient. The formulations and recommended dosages of hormones can be found in the feminizing and masculinizing hormone therapy sections.
Discuss the potential costs of hormone therapy
Costs for medications (for those without drug coverage) vary and are listed in the feminizing and masculinizing hormone therapy sections. Certain formulations are covered for patients on the Ontario Drug Benefit program (see below).
Fertility preservation is not presently covered by OHIP. Currently, some hospital-based clinics such as Mount Sinai Hospital’s Centre for Fertility and Reproductive Health in Toronto, ON, may offer a discounted rate for medically necessary gamete preservation and subsequent fertility treatment, such as in the case of gender transition. If indicated, referral to a fertility clinic should be initiated early in the hormone planning period as this process takes time. Care should be taken to refer patients for fertility services at centres that have experience working with trans people whenever possible.
Relevant especially to transfeminine patients since hormone administration may slow the growth of hair, but not substantially reduce the amount of facial (or other body) hair. As such, laser treatments and/or electrolysis are often required. These services are not presently covered by OHIP and it can be a challenge to find a provider who is both sensitive to the trans patient and able to work within fixed budgets. Permanently eliminating the bulk of facial hair may cost up to several thousand dollars and this should be discussed up-front and considered in the timeline of the patient’s medical and social transition.
A list of providers with knowledge and experience working with LGBT2SQ individuals may be found through Rainbow Health Ontario’s online service directory
Submit Exceptional Access Program (EAP) form for patients on Ontario Drug Benefit (ODB)
Patients covered by the Ontario Drug Benefit (ODB) program include those on Ontario Works (OW), the Ontario Disability Support Program (ODSP), seniors ≥65 years of age, youth ≤24 years of age without private insurance (via OHIP+) and those on the Trillium Drug Program. For patients on ODB, injectable testosterone is covered with the submission of an Exceptional Access Form (EAP), while anti-androgens and estradiol are covered without the need for EAP approval.
We suggest submitting the EAP application early in the process of planning given that the processing time by the Ministry of Health and Long-Term Care can vary. Approval does not commit the provider to prescribing hormone therapy but prevents undue delays once the planning period is complete.
Recommendation: Injectable testosterone is funded by the Ontario Drug Benefit (ODB) program for gender affirmation with an Exceptional Access Program (EAP) request. We suggest that providers submit EAP requests for both testosterone cypionate and testosterone enanthate, so that delays in access do not result when one formulation is on back order or not locally available. (See Appendices N and O in the Guidelines for samples).
-
Sample Request for an Unlisted Drug Product, Testosterone Enanthate (Delatestryl)
-
Sample Request for an Unlisted Drug Product, Testosterone Cypionate (Depo-Testosterone)
Risk management
Have precautions been optimally managed or is a management plan in place?
Each hormone will have its own specific considerations and precautions which are explained in more detail in the feminizing and masculinizing hormone therapy section of this guide. However, it is worthwhile to address general considerations and precautions with hormone use.
Keep in mind
Denying access to hormones can do much more harm than the possible risks of treatment. With an informed-consent approach (support, education and consent) many providers will initiate hormones with individuals with higher risk profiles when it increases their quality of life/chance of survival greatly.Lifestyle considerations
The initiation of hormone therapy and the expectation of aligning one’s body with an internal sense of gender may create an opportunity for a patient to begin to develop a new relationship with their body and initiate lifestyle changes that positively impact health. We have often witnessed this time of transition provide the impetus and inspiration for lasting positive lifestyle changes.
Smoking and obesity will increase the risks associated with hormone therapy. It is worthwhile for the provider and patient to work to decrease these risks as much as possible, with the understanding that this is not always feasible before starting treatment, and a harm reduction approach may be necessary. Substance use disorders – whether involving alcohol, street or prescription drugs – may introduce additional risks that should be considered. In the Toronto area, COMPASS at CAMH provides counselling and treatment services.
Mental health considerations
Trans patients invariably experience some degree of minority stress. Adapting Meyer’s definition in relation to lesbian, gay and bisexual populations,1 minority stress in the trans population may be thought of as: the chronic psychological strain resulting from stigma and expectations of rejection and discrimination; decisions about disclosure of gender identity; and the internalization of transphobia that trans people face in a cis-sexist society.
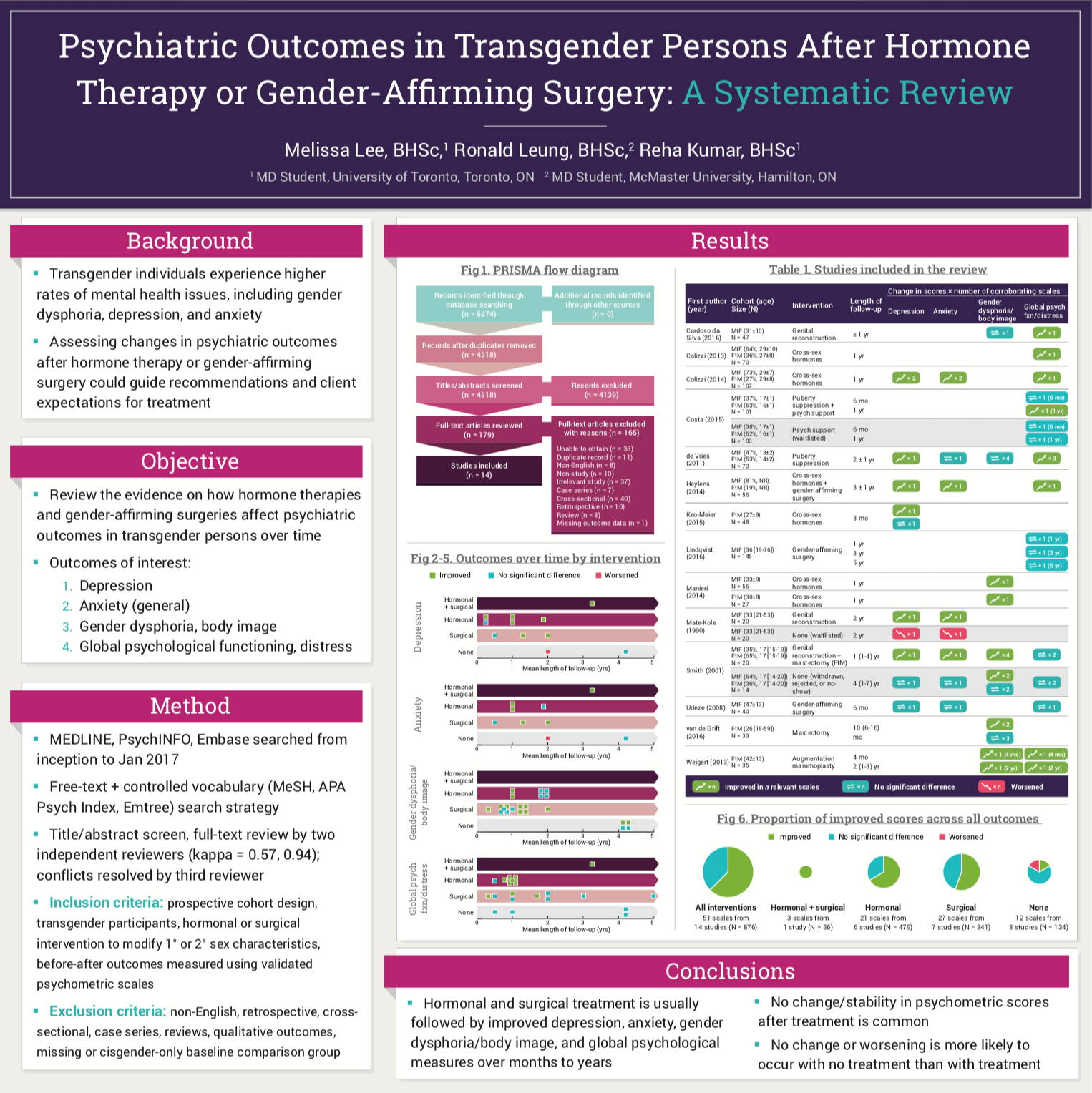
Not surprisingly, trans and non-binary people have a higher prevalence of mental health conditions that are related to stress (such as depression, anxiety, and substance abuse). The presence of mental health concerns does not preclude access to hormone therapy, rather, according to WPATH, these concerns should ideally be 'reasonably well controlled prior to or concurrently with hormone therapy'. There is no convincing evidence that hormone therapy is associated with the onset or worsening of mental health conditions, in fact, a number of studies have demonstrated consistent improvements in psychological functioning. Nonetheless, it may be prudent to exercise some caution in patients with bipolar disorder or psychotic disorders, particularly when sub-optimally managed.
Primary Care Providers can assist patients in the optimization of mental health conditions in preparation for and throughout medical transition
View suggested mental health considerations for periodic review by Collaborative MD and Nursing Team
Source:
- Psychiatric Outcomes in Transgender Persons After Hormone Therapy or Gender-Affirming Surgery: A Systematic Review. Lee M, Leung R, Kumar R. Poster Presentation. University of Toronto | McMaster University. 2019
For those with complex, severe, or poorly controlled mental health conditions, a referral to a specialized centre such as the CAMH Adult GIC or other psychiatrist with experience working with trans patients can be helpful.
Although acute suicidality has previously been considered a contraindication to hormone administration (particularly testosterone), there may be cases where a patient who is at significant risk of suicide, but is able to provide informed consent may in fact benefit greatly from the initiation of hormone therapy. This may be particularly true when intense gender dysphoria is the main source of the psychological distress experienced by the patient.
We suggest that these types of situations may be best approached on a case-by-case basis, with an assessment of the risks and benefits of hormone provision in relation to the individual patient’s mental health. There may be situations in which the best course of action would be to start the patient on low-dose therapy while strategizing around suicide risk reduction, for example by establishing a crisis plan and connecting the patient with additional mental health support. If a patient is experiencing a major depressive episode, pharmacotherapy for clinical depression should be discussed.
Differential diagnosis
Other possible diagnoses
Rule out other possible diagnoses (e.g. schizophrenia and other psychotic disorders, dissociative disorder and body dysmorphic disorder). Such diagnoses are rarely found to be underlying the desire for gender-affirming treatment, but can occur and thus should be ruled out. If the presentation is unclear, it is appropriate to obtain the opinion of a psychiatrist who is experienced in working with trans people if possible.
Ensure there is no evidence of an intersex condition.
Previously, genital examination was recommended prior to hormone initiation; however we suggest that inquiry into any history suggestive of an intersex condition (e.g. ambiguous genitalia, unexpected pubertal changes for sex assigned at birth) along with baseline hormone levels within expected ranges are sufficient. Findings suggestive of an intersex condition merit further investigation and/or consultation with an endocrinologist prior to treatment.Does the patient meet the criteria for gender dysphoria/gender incongruence?
The provision of hormone therapy has generally been preceded by a diagnosis of Gender Dysphoria as outlined in the Diagnostic and Statistics Manual, Volume 5 (DSM-5). There has been a great deal of debate in both the medical and trans communities around the appropriateness of using a psychiatric diagnosis (or a diagnosis at all) for trans individuals. The aim to destigmatize gender diversity while securing access to appropriate treatment has been a central dilemma in this debate.
The revision of the diagnosis (previously called Gender Identity Disorder) and associated diagnostic criteria in 2013’s DSM-5 represented a step towards depathologizing gender difference and validating the spectrum of gender identities.
The WHO has taken a step further towards the depathologization of trans identities in their International Statistical Classification of Diseases and Related Health Problems (ICD-11). They have renamed the diagnosis Gender Incongruence and removed the diagnosis from the category of mental health disorders, placing it instead in a category of “Conditions Related to Sexual Health.”
View criteria for the DSM-5 diagnosis of Gender Dysphoria
Harm reduction: Fast-tracking through the planning period
Provision of hormone treatment may be undertaken, in some cases, without completing all of the usual tasks of the planning period. Situations that may warrant a degree of ‘fast-tracking’ through the planning period include:
- A patient who is already using hormones without a prescription
- A patient who has marked distress regarding their gender presentation
- The patient's medical and/or gender history are well known prior to the patient seeking hormone therapy
- If another knowledgeable provider has recently performed part or all of the assessment and the associated records are available for review or a conversation with the prior provider can be arranged, all tasks of the assessment period need not be repeated